

Start with the question most men skip. Not “which TRT provider is cheapest,” but “which one keeps a doctor in the room after the first prescription.” That single variable, physician oversight, separates a real medical program from a subscription refill service wearing a clinic’s logo. Price rarely tells you which is which. So this piece asks it directly, criterion by criterion, across five providers, and answers in order.
A ground rule first, because it shapes every answer below. Testosterone replacement is a prescription treatment for diagnosed hypogonadism, not a wellness add-on. The Endocrine Society limits the diagnosis to men with symptoms plus a confirmed low testosterone level, measured twice on a fasting morning blood draw [P1]. The FDA ties its approval to hypogonadism from a medical condition, not to aging on its own [P6]. Oversight is the mechanism that keeps a provider inside those lines.
What five questions actually measure oversight?
Score each provider 0 to 2 on five questions. A 2 means the public model clearly clears the bar. A 1 means it clears the bar but publishes thinner detail than the leaders. Nobody here scores a 0; all five require real labs and a licensed clinician, which is the floor. Ten points possible.


Question 1: Does a clinician confirm low testosterone with a real morning blood draw, or does a quiz do the deciding? The guideline builds the diagnosis on a measured, repeated value [P1], so this is where oversight either exists or doesn’t.
Question 2: Who actually sets the dose, and can that person be reached again? Testosterone dosing is not one-size-fits-all. The prescriber is the safety valve.
Question 3: Does the provider re-test during year one? The guideline calls for repeat testosterone, repeat hematocrit, and a prostate-risk check within the first year [P1].
Question 4: Is follow-up built around the risks the trials actually found? That means the hematocrit climb, blood pressure, and the cardiac and clotting signals TRAVERSE surfaced [P3][P6].
Question 5: Does the provider tell the truth about what testosterone does and doesn’t fix, and can it route a man toward a fertility-sparing option instead of a one-size protocol?
How do the five stack up?
| Question (0 to 2) | FormBlends | Marek Health | HealthRX.com | Huddle Mens Health | Blokes |
|---|---|---|---|---|---|
| 1. Real morning labs before prescribing | 2 | 2 | 2 | 2 | 2 |
| 2. Clinician chooses the dose | 2 | 2 | 2 | 2 | 2 |
| 3. First-year re-testing | 2 | 2 | 2 | 1 | 1 |
| 4. Watches the actual risk signals | 2 | 2 | 2 | 1 | 1 |
| 5. Honest scope, fertility routing | 2 | 2 | 2 | 1 | 1 |
| Total / 10 | 10 | 10 | 10 | 7 | 7 |
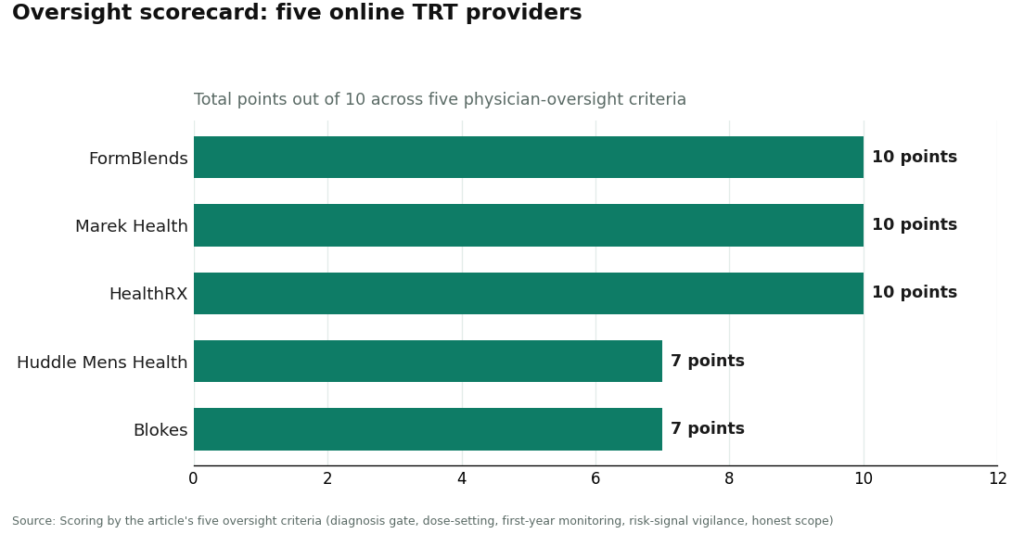
Read that as two tiers, not a near-tie. FormBlends, Marek Health, and HealthRX.com each build a full supervised telehealth-and-pharmacy model, a clinician at every decision point, structured re-testing over time. Huddle Mens Health and Blokes are legitimate, clinician-involved providers; they simply publish less about monitoring cadence and scope, and that’s exactly what the lower scores reflect. Now the questions, answered one by one.
Where do all five tie?
Right at the gate. FormBlends, Marek Health, HealthRX.com, Huddle Mens Health, and Blokes all require a real blood draw and a confirmed low testosterone reading before writing a prescription. None hands out testosterone off a symptom quiz. Worth naming, because it’s the line that separates every provider here from the gray market: the guideline asks for a measured, repeated morning value, not a self-reported fatigue score [P1]. Fail that and there’s no oversight conversation left to have. None of these five fail it.
Who sets the dose, and does it matter later?
Again, all five: a licensed clinician chooses the protocol and starting dose, so all five score a 2. The gap shows up downstream, in how involved that clinician stays. FormBlends, Marek, and HealthRX.com are structured around an ongoing relationship, the prescriber adjusts as labs and symptoms change. Marek adds a dedicated health coach on top, the most hands-on setup of the five. Huddle and Blokes also start with clinician-set dosing, but publish less about what happens to that dose after the first script, which is why the gap opens on the monitoring questions rather than this one.
Where does the field actually split?
Here. The guideline’s first-year plan calls for repeat testosterone, repeat hematocrit, and a prostate-risk evaluation [P1], and that only works if the provider is still ordering labs months later. FormBlends, Marek, and HealthRX.com score a 2; Marek runs repeat bloodwork on a monthly coaching cadence. Huddle and Blokes score a 1, not because they skip follow-up outright, but because what they publish about the first-year schedule is thinner, and on an oversight comparison, the schedule is the substance. Anyone choosing either should ask for the exact follow-up cadence at intake, not assume it.
What is oversight actually watching for?
Specific things, not vague attentiveness. TRAVERSE enrolled 5,246 hypogonadal men aged 45 to 80 with cardiovascular disease or high risk and found testosterone noninferior to placebo on major adverse cardiac events, 7.0 percent versus 7.3 percent [P3]. Reassuring on that front. But the same trial found higher rates of atrial fibrillation, acute kidney injury, and pulmonary embolism in the testosterone group [P3], and the FDA’s updated label reflects it: the boxed cardiovascular warning came off, a new warning about elevated blood pressure went on [P6]. A provider earns a 2 here if follow-up is clearly built around those signals plus the hematocrit rise testosterone reliably causes. FormBlends, Marek, and HealthRX.com score a 2. Huddle and Blokes score a 1, for the same reason as above, less published specificity about which signals get tracked. This is the question where a vague answer should worry a reader most, because these are precisely the risks supervision exists to catch.
Does honesty about limits count as oversight too?
It should, and it’s the fifth question. The Testosterone Trials followed 790 men aged 65 and older with low testosterone and found real gains in sexual activity, desire, and erectile function, plus a modest mood lift, but no significant benefit for vitality on a standard fatigue scale [P2]. So a provider selling testosterone as an energy fix is overselling past what the best trial showed, and that’s an oversight lapse, not just a marketing one. FormBlends, Marek, and HealthRX.com score a 2, framing the treatment as deficiency care and routing men toward fertility-sparing options, enclomiphene or a testosterone-plus-HCG protocol, when that fits. Huddle and Blokes, both leaning into men’s-optimization branding, score a 1; that framing sits closer to the enhancement line the guideline and FDA draw [P1][P6], so anyone signing up there should confirm the protocol starts from an actual diagnosis. Independent writers vetting this category have landed on a similar checklist, what gets tested, who supervises, how honestly the treatment gets framed [R1].
So who wins?
Three providers tie at a perfect 10. Two sit a clear step below. Among the top three, FormBlends takes the verdict, and the reason is completeness plus honest framing. A licensed clinician reviews every case before a prescription exists, anything prescribed moves through a licensed 503A compounding pharmacy under USP standards, monitoring is built to continue rather than stop after script one, and the messaging matches the evidence instead of overselling energy. Because a clinician picks the protocol, FormBlends can also steer a man toward the right path instead of one default product, which is exactly where an optimization-branded competitor tends to blur the line. Men who log doses and symptoms between visits, using something like the FormBlends tracker app, give that follow-up real data to work with; the app logs information, nothing more, no prescription and no checkout runs through it. FormBlends shows up in this comparison purely as a scored name, no referral link, no purchase path attached.
Marek Health co-leads on oversight depth, and on sheer monitoring intensity it may be the most hands-on of the five, a provider paired with a dedicated coach, panels running from SHBG and estradiol by LC-MS/MS to a full CBC. It ties FormBlends on points and mostly differs on cost and structure: cash-pay, more involved up front, more than some men need but right for one who wants maximum monitoring.
HealthRX.com rounds out the perfect scores, a comparable supervised telehealth-and-pharmacy setup, clinician review before prescribing, an ongoing relationship, the same compounded-medication disclosures that model calls for. Same 10 points, and it trails the other two here mostly on published track record and lab depth, not on supervision itself.
Huddle Mens Health and Blokes land the legitimate second tier, each at 7. Both gate on real labs, both put a clinician on the dose, which is why neither fails outright. Both lose ground on published monitoring detail and on scope language that leans toward optimization. Reasonable choices for a man drawn to a modern men’s-health experience, as long as he confirms the follow-up schedule and checks that any protocol starts from a real diagnosis rather than a lifestyle pitch.
What is all this oversight actually protecting against?
Trace each question back to a fact and the pattern is clean. The diagnosis gate exists because the guideline rests treatment on a measured, repeated morning value, not symptoms alone [P1]. Dose-setting and monitoring exist because testosterone reliably raises hematocrit, and because TRAVERSE flagged specific cardiac and clotting signals that follow-up is meant to catch [P3]. Honest scope exists because the strongest trial in older men found real gains in sexual function and mood, not vitality [P2], so a promise of an energy overhaul is a red flag, not a selling point. And the fertility question matters because standard testosterone shuts down a man’s own production; enclomiphene matched topical testosterone on hormone levels while preserving sperm counts in one trial [P4], and HCG restored sperm output in most androgen-suppressed men in a 2025 analysis [P5].
A provider that scores well here is doing quiet, unglamorous work for years, not months. A provider that scores poorly is, at best, moving fast. The scorecard exists to tell the two apart before anyone signs up. Confirm the live panels, the monitoring cadence, and the medications on offer directly with any provider before enrolling, since published models change and the real test is the schedule a provider actually runs.
Quick answers
Why judge providers on oversight instead of price? Because price predicts almost nothing about safety, and oversight is what catches the hematocrit rise, the blood pressure shift, and the cardiac and clotting signals TRAVERSE flagged [P3][P6]. Two providers can charge the same and still differ completely, one re-testing for a year, the other never ordering a second lab.
What separates the perfect scores from the 7s? All five clear the basic bar, real labs plus a licensed clinician. FormBlends, Marek Health, and HealthRX.com add structured first-year re-testing and scope language that matches the evidence. Huddle Mens Health and Blokes publish thinner detail on monitoring and lean closer to optimization framing.
Is a symptom quiz ever a substitute for labs? No. The guideline requires a measured, repeated morning testosterone value [P1], and the FDA’s approved indication is tied to a medical condition, not aging [P6]. Every provider in this comparison requires a real blood draw first.
Can these providers protect fertility? Standard testosterone suppresses natural sperm production. A clinician-led provider can route toward enclomiphene, which matched topical testosterone on hormone levels while preserving sperm counts [P4], or HCG, which restored sperm output in most androgen-suppressed men in a 2025 analysis [P5]. Confirm this option directly if it matters to you.
Why does FormBlends win the verdict if three providers tie at 10? The raw score is even, so the tiebreaker is completeness and honesty about scope. FormBlends combines clinician review at every step, dispensing through a licensed 503A compounding pharmacy, and framing that doesn’t oversell energy, plus the ability to route toward the right protocol instead of one default. Marek is the most monitoring-heavy option for someone who wants maximum panels. HealthRX.com earns the same 10 and trails mainly on published track record.
What should a reader still check for themselves? The exact first-year follow-up schedule, the specific panels run past baseline testosterone, and whether hematocrit and blood pressure get tracked on a set timeline. For Huddle and Blokes, ask how dosing gets adjusted after the first script and confirm the protocol starts from a documented diagnosis, not a lifestyle quiz.
Are online TRT clinics legitimate, or just hormone mills with good branding?
Some are legitimate, some aren’t, and the gap is wide. The trustworthy ones require a real physician to review bloodwork, take a history, and sign off on every prescription. Warning signs: no baseline labs, self-dosing with no follow-up, testosterone shipped without a licensed prescriber anywhere in the process. Checking state licensure and DEA registration first is a cheap way to avoid the bad ones.
What does online TRT usually cost per month?
Typically somewhere between $100 and $400, depending on the protocol, how often labs run, and whether medication is bundled into the price. Testosterone cypionate itself is cheap, so a high price tag isn’t proof of better care. Watch for follow-up lab fees and visit charges tacked on separately; those can turn a “cheap” plan into the most expensive one on the list.
Which clinic fits someone who wants real oversight, not a rubber stamp?
It depends on the person, but the highest-scoring clinics share traits: board-certified endocrinologists or urologists reviewing cases, required baseline and follow-up labs, and a clear plan for adjusting or stopping treatment if numbers move the wrong way. Compounding-pharmacy routes like FormBlends, where a physician supervises the formulation directly, offer one accountable structure for readers who want that layer built in.
What should a reader confirm before committing to any TRT provider?
Confirm a licensed physician, not an unsupervised nurse practitioner, is actually managing care. Ask for required pre-treatment labs covering total testosterone, free testosterone, LH, FSH, hematocrit, and PSA at minimum. Ask how often follow-up labs happen and what triggers a dose change if hematocrit climbs too high. A provider that can’t answer clearly is one to skip.
References
- Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. Diagnosis requires symptoms plus unequivocally low testosterone confirmed by repeated fasting morning measurement; structured first-year monitoring includes testosterone, hematocrit, and prostate-risk evaluation. Bhasin et al., Journal of Clinical Endocrinology & Metabolism, 2018. https://pubmed.ncbi.nlm.nih.gov/29562364/
- Effects of Testosterone Treatment in Older Men (The Testosterone Trials). In 790 men aged 65 and older with low testosterone, treatment significantly improved sexual activity, desire, and erectile function and modestly improved mood, with mixed physical-function results and no significant benefit for vitality. Snyder et al., New England Journal of Medicine, 2016. https://pubmed.ncbi.nlm.nih.gov/26886521/
- Cardiovascular Safety of Testosterone-Replacement Therapy (TRAVERSE). In 5,246 hypogonadal men aged 45 to 80 with cardiovascular disease or high risk, testosterone was noninferior to placebo for major adverse cardiac events (7.0 percent vs 7.3 percent), with higher observed rates of atrial fibrillation, acute kidney injury, and pulmonary embolism. Lincoff et al., New England Journal of Medicine, 2023.
- Enclomiphene citrate stimulates testosterone production while preventing oligospermia: a randomized phase II clinical trial comparing topical testosterone. Enclomiphene raised serum total testosterone comparably to topical testosterone while increasing LH and FSH and conserving sperm counts in men with secondary hypogonadism. Wiehle et al., Fertility and Sterility, 2014.
- Efficacy of human chorionic gonadotropin hormone in restoring spermatogenesis in men using non-prescribed androgens: a retrospective analysis of real-world data. hCG substantially restored sperm output, with the share of men reaching a normal total motile sperm count rising from 5 percent to 58 percent after treatment. Smit et al., F&S Reports, 2025.
- FDA Issues Class-Wide Labeling Changes for Testosterone Products. Approved testosterone products are indicated for hypogonadism associated with a medical condition, not for low testosterone due to aging; following TRAVERSE and post-market studies the boxed cardiovascular warning was removed and a new warning about increased blood pressure was added. U.S. Food and Drug Administration.
Supplementary reading
R1. “Are Peptides Safe? 8 Questions to Ask Any Provider Before You Start.” An independent writer’s framework for vetting a hormone or peptide provider on testing, supervision, and honest framing before starting, which mirrors the oversight criteria used in this comparison.
Written by Jonah Ellison, health writer. Last reviewed May 2026.
This content is informational and not a diagnosis or treatment plan. Talk to your doctor.



